First clean water, now clean air
Published 30 April 2023 ⋅ Comment on EA Forum
Back to writingContents (click to toggle)
7,175 words • 36 min read
(sidenote: By Gavriel Kleinwaks, Alastair Fraser-Urquhart, Jam Kraprayoon, and Josh Morrison) from Rethink Priorities and 1Day Sooner was my main source for this (here’s a summary). Many of the substantial points I make are taken from it, though errors are my own. It’s worth reading!
You can also listen to an AI narration of this article, below:
Clean water
In the mid 19th century, London had a sewage problem. It relied on a patchwork of a few hundred sewers, of brick and wood, and hundreds of thousands of cesspits. The Thames — Londoners’ main source of drinking water — was near-opaque with waste. Here is Michael Faraday in an 1855 letter to The Times:
Near the bridges the feculence rolled up in clouds so dense that they were visible at the surface even in water of this kind […] The smell was very bad, and common to the whole of the water. It was the same as that which now comes up from the gully holes in the streets. The whole river was for the time a real sewer […] If we neglect this subject, we cannot expect to do so with impunity; nor ought we to be surprised if, ere many years are over, a season give us sad proof of the folly of our carelessness.

That “sad proof” arrived more than once. London saw around three outbreaks of cholera, killing upwards of 50,000 people in each outbreak.

But early efforts to address the public health crisis were guided by the wrong theory about how diseases spread. On the prevailing view, epidemics were caused by ‘miasma’ ((sidenote: The same idea gave us the word ‘malaria’, also literally ‘bad air’ through medieval Italian)) — a kind of poisonous mist from decomposing matter. Parliament commissioned a report on the ‘Sanitary Condition of the Labouring Population’, which showed a clear link between poverty and disease, and recommended a bunch of excellent and historically significant reforms. But one recommendation backfired because of this scientific misunderstanding: according to the miasma theory, it made sense to remove human waste through wastewater — but that water flowed into the Thames and contaminated it further.
But in one of these outbreaks, the physician John Snow has spotted how incidence of cholera clustered around a single water pump in Soho, suggesting that unclean water was the major source of the outbreak. A few years later, the experiments of Louis Pasteur helped foster the germ theory of disease, sharpening the understanding of how and why to treat drinking water for public health. These were well-timed discoveries —
Because soon things got even worse. Heat exacerbated the smell; and the summer of 1858 was unusually hot. 1858 was the year of London’s ‘Great Stink’, and the Thames “a Stygian pool, reeking with ineffable and intolerable horrors” in Prime Minister Disraeli’s words. The problem had become totally unignorable.
Parliament turned to Joseph Bazalgette, chief engineer of London’s Metropolitan Board of Works. Spurred by the Great Stink, he was given licence to oversee the construction of an ambitious plan to rebuild London’s sewage system, to his own design. 1,800km of street sewers would feed into 132km of main interconnecting sewers. A network of pumping stations was built, to lift sewage from streets below the high water mark. (sidenote: Much of these facts are from The Good Ancestor (2020)), the result was the kind of modern sewage system we mostly take for granted: a system to collect wastewater and dump it far from where it could contaminate food and drinking water; in this case a dozen miles eastwards to the Thames estuary. "The great sewer that runs beneath Londoners”, wrote Bazalgette’s obituarist, “has added some 20 years to their chance of life”.
Remarkably, most of the system remains in use. London’s sewage system has obviously been expanded, and wastewater treatment is much better. Bazalgette’s plan was built to last, and succeeded.
{kind=link}
As London built ways of expelling wastewater, it also built ways of channelling clean and running drinking water. New canals, plumbing infrastructure, and water supply companies piped water from springs, wells, and rivers straight into houses and public drinking fountains; replacing wells, collecting rainwater, or unclean water pumps.
One of the nice things about living in London today is that it is very, very easy to find running water, and it’s reasonable to basically never worry about whether the water that comes out of taps is safe to drink. In the last century, 7 people have died of cholera in the United Kingdom.
The same story unfolded nearly everywhere in the developed world, and it marked the beginning of a so far effectively permanent end to waterborne disease in wealthy countries. I naively but conservatively estimate clean water measures saved more than 130 million people in the 50 years (sidenote: The Global Burden of Disease estimates that unsafe water sources are still responsible for 1.2 million deaths each year. Very roughly three quarters of the world have access to a clean water source, and 6% of the world population did not have access to an improved water source of any kind. So let’s conservatively guess that clean water measures reduce the deaths attributable to unsafe water by 75%, compared to a world with the same population but no clean water technology, on average from 1973 to the present day (i.e. over the last 50 years). In other words, we’re guessing that without clean water measures, deaths from unsafe water would be $1.2 million / (1-75%) = 4.8 million and so counterfactual lives saved per year is 4.8-1.2 = 3.6 million per year. Average world population over that period was about 75% of today. So a naive and conservative guess at the lives saved from clean water measures = 75% × 3.6 million × 50 = 135 million people.). Of course these improvements to sewage and plumbing and water treatment were expensive, but very clearly paid for themselves many times over, and it is clearly worth expanding those measures until everyone in the world has access to them.
That’s not mentioning the improvements from sanitation and hygiene, which are different from just having access to clean drinking water. Unsafe sanitation and lack of access to handwashing facilities, treated as risk factors, together look responsible for nearly 1.5 million additional deaths annually.
I just think this is worth dwelling on: in about half a century, developed countries effectively ended waterborne disease.
Clean air
You probably guessed from the title but the punchline is that now’s a good time to do the same thing with airborne disease.
The basic analogy:
- Unclean water imposed an enormous human toll, until we built ways to deliver clean water, dispose of unclean water, and keep the two separated. Now nearly everyone in at least developed countries has access to safe drinking water, and in those places most waterborne diseases are very rare.
- Unclean indoor air continues to impose an enormous human toll, even in developed countries. Almost nowhere in the world do we adequately treat, monitor, or even circulate the air we breathe: we breathe untreated air pretty much all the time. But we know how to build measures to effectively end airborne diseases, too.
I think the first step here is just noticing the price we pay for unclean indoor air. Consider: most people just have to factor in a ~single digit number of days per year recovering from some airborne disease like the flu or common cold. In the US alone, this costs double-digit billions of dollars in direct healthcare costs and foregone wages. Ventilating air helps to eliminate biological pathogens, but it also just makes it fresher and less stuffy — where some studies tentatively show double digit percentage improvements in productivity from just getting rid of stuffy (CO2-rich) air. But likely the biggest cost is now also the most obvious. Every few decades a pandemic with airborne transmission pathways will tear through the world, and the world will be mostly powerless to stop it. The most recent example took around 20 million lives so far. The next could be even worse.
Part of the problem with making these facts salient might be that our disgust reactions aren’t firing in helpful ways: unclean water is visibly (and olfactorily) unclean, but bad air is perfectly disguised as clean air, and (sidenote: Obviously this changed some during the pandemic. For instance, sitting in a packed subway train (without a mask) still feels mildly stressful.). So the first step is bringing the human costs of unclean air (sidenote: Lizka on the EA Forum points out that this suggests a potential for advocacy through visualisations which make the mechanisms of unclean air visually salient. This NYT piece is a great example.).
In the hopeful story, these costs become historical. Covid could be to airborne diseases like London’s cholera outbreaks and Great Stink were to waterborne diseases: a confluence of (i) “wow, as long as we know how to end this, we should”; and (ii) “huh, looks like we do increasingly know how to end this”.
I don’t know whether that is the story we’re in, but I think we know enough to describe many of the practicalities. So here’s how the hopeful story could play out, across a handful of technologies:
The high-level plan
We’ll focus on indoor air quality, because respiratory pathogens are much (sidenote: Largely because indoor spaces are more crowded. This study estimates more than 90% of Covid infections occurred indoors.) (and treating indoor air is achievable and affordable).
The world we want to end up in is a world where we massively slow the spread of airborne pathogens, primarily to reduce the vast expected cost of catastrophic biorisk, and also to reduce the yearly toll of (non-pandemic) respiratory diseases.
How do we reach that point of safety? Practically, we’ll need technology that does two things. Either: straightforwardly blocking the spread of pathogens in crowded indoor spaces. If patient zero coughs, and the aerosolized pathogen is sterilised or ventilated away before it can spread to anyone else, then a potential outbreak is stopped dead. Or, at least: slowing transmission. If Rt drops and stays below 1, you don’t have the conditions for an epidemic. And in any case, slowing transmission buys time for other medical countermeasures — like the time to develop and deploy vaccines.
On a social level, we’ll need ways to make sure these safety-promoting technologies are deployed as widely, cheaply, and quickly as they need to be. With two tools: (i) standards and other regulations to capture the externalities from unclean air; and (ii) major R&D initiatives like prizes, FROs, or advanced market commitments to speed up wide rollouts of these safety-promoting technologies.
Which technologies?
Ventilation
Ventilation just means getting rid of the stale air in a room and replacing it with air from outside the room. If the air from outside the room is cleaner, then you’ve now got cleaner air.
This metaanalysis finds strong evidence that ventilation helps reduce infection rates. There’s also some evidence for more general health benefits, like less inflammation, sick leave, and fewer asthma and allergy symptoms.
The V in HVAC is ventilation, so many AC / heating systems ventilate air already. A DIY version of a ventilation system is to open two roughly opposite windows in a space, and place a fan moving air out one of the windows.
There are some drawbacks: it’s often noisy, often energy-consuming, and it relies on outdoor air being significantly fresher than indoors, which isn’t always the case (especially in cities).
Filtration
Then there’s filtration: passing air through a filter to remove small particles, including pathogens. Quoting from this Rethink report on indoor air quality:
Standalone filtration units […] have been shown to reduce the exposure to pathogenic aerosols under controlled conditions, with 5 eACH HEPA filtration in classrooms enough to cause a 4-5 fold drop in pathogen dose.
[…] Addition of filters to existing ventilation systems in a typical model scenario has been shown to reduce relative risk of infection of influenza by up to 47%, at a total annual cost of $352 for HEPA filters[.]
[…] In addition to reducing pathogen transmission, filtration has benefits for respiratory health and cognition, due to its ability to remove harmful particulate, gaseous, and chemical pollutants. Given these benefits, widely investing in improved filtration in built environments is likely to help the population even in non-pandemic years.
The way filters work — even the advanced ones — is almost embarrassingly simple. Get some kind of foamy/spongy/fibrous material with lots of small holes; put many layers of that material into a box; and force air through that box with a fan. During the pandemic, Richard Corsi proposed a design for a DIY air purifier which is more or less as simple as I made out, enabling people to cheaply build their own air purifiers for homes and schools and offices. It’s called the Corsi-Rosenthal box, and it takes about $100 and 15 minutes to build. Here is Corsi in a radio interview: “People are now reporting 600 cubic feet per minute (280 L/s) in clean air delivery rates. That’s phenomenal. That’s actually better than a lot of the more expensive HEPA-based portable air cleaners”. Even more than ventilation systems, air filters are low-tech, and already very cheap to install and maintain (I’d guess typically less expensive than fire safety systems).
An aside: ventilation plus filtration is the major reason that the risk of Covid infections on flights was and is so relatively low: air in the cabin is replaced every couple minutes, fresh air is drawn from outside the plane, and mixed with recycled air passed through HEPA filters. Airbus says that the risk of infection is lower on a plane than people sitting six feet apart in an office.
Germicidal UV (GUV)
Like antibacterial soap, it turns out that certain wavelengths of light can effectively sterilise pathogens (without sterilising humans). There are roughly two kinds:
Upper-room UVC illuminates the top of the room and avoids illuminating people. This means you can use relatively lower frequencies of UV light which are currently easier to produce with lamps, but which can cause eye damage in humans. Upper-room UVC is cheap and well-understood. This study found an 80% reduction in TB transmission in guinea pigs. So it will also keep pets safe.
Far-UVC is a narrow band of UV wavelengths at higher frequencies than are currently economical to produce with lamps. The key advantage of Far-UVC is that early studies show no indications that it harms humans, even at very high doses. But it is effective at stopping pathogens: for example this study finds that Far-UVC light inactivated 99.9% of aerosolized coronaviruses. As long as longer-term studies on the safety of Far-UVC agree, then this is some extremely exciting technology.
Currently, Far-UVC is too expensive to scale to a significant fraction of all the indoor spaces in a country. And current versions produce small amounts of a kind of smog that can be harmful (without attendant ventilation). So I’m not advocating for installing current UVC tech in every room — we’ll need a few years of figuring out how to produce it more cheaply and with fewer side-effects (ideally with LEDs).
In the hopeful story, new PhDs and R&D labs begin a concerted program to first make the breakthroughs which would enable Far-UVC to become cheap, and then major manufacturers introduce the technology to wider and wider markets. It might parallel the (sidenote: In a nutshell: (1) Solar cells were pioneered in R&D labs, often backed by governments. E.g. the US wanted to put solar cells on spacecraft; (2) Then they began being sold to private buyers in niche markets. E.g. Japan subsidised solar cells for calculators, toys, and watches; (3) Then Germany began a major subsidy program to develop domestic solar power capacity in the early 2000s; (4) Then other manufacturers took the grid energy solar tech and drove down costs through building a ton of it; especially in China. As a result, between 1975 and 2021, the cost of a watt of solar energy fell by more than 40,000%; and by more than 600% in the past decade alone. Solar PV also did not majorly benefit from philanthropic funding, in the form of e.g. prizes or advanced market commitments. So it’s a story which demonstrates how costs can fall quickly and dramatically with (i) major investment and (ii) the ability to learn from building millions of units (unlike e.g. nuclear power plants). Both those factors can apply to Far-UVC, and we have the option to supercharge the process with early incentives.) between 1975 and 2021, the cost of a watt of solar energy fell by more than 40,000%; and by more than 600% in the past decade alone. The process from now to real maturity — where Far-UVC is cheap enough to be ubiquitous — needn’t last much longer than Bazalgette’s 18-year sewage project.
Standards and monitoring
The expectation of clean water in wealthy countries is enabled by technology and infrastructure; like effective sewage systems and water treatment facilities. But to a large extent it is also enabled, and was initially bootstrapped, by sound policymaking and regulation.
Regulation requires verification. In the UK the Water Supply (Water Quality) Regulations 2016 say things about how much lead can be in my tap water (< 10µg/litre), and water test kits exist to check for lead concentrations, giving those regulations teeth. Similarly, UK building standards say things about how new builds should handle drainage and waste disposal and other exciting things, all easily verifiable.
So is it easy to measure air quality? Pretty much. The concentration of CO2 in a room can be a good proxy for how well ventilated it is (and therefore for risk of transmission without filtration or germicidal light). Plus, CO2 buildup itself can be cognitively impairing. CO2 monitors can cost less than $20. Only a notch more expensive are gauges for different sizes of particulates. Again, particulate matter in general can both proxy well for the effectiveness of filtration, and cause breathing problems of their own. Metagenomic sequencing technology could also survey the air for actual pathogenic material, but it needs to (sidenote: There will presumably be a point where the sequencing technology is affordable enough to be used in some government standards, but too expensive to be permanently installed in most businesses / buildings / homes. In this case, you could imagine inspectors who visit on the order of every couple years to take samples of air from buildings, and mandate changes (e.g. some government subsidised filtration system) if the readings are bad (analogous to fire safety inspections).). So we have multiple easy ways to measure air quality, which is good news for straightforward, boring, scalable kinds of (sidenote: One nice common feature of having widespread air quality measurement is that people can learn instincts and norms around improving air quality. For instance, some people who use CO2 monitors eventually become more sensitive to when a room feels ‘stuffy’, and when a room appears poorly ventilated such that they can expect it will feel stuffy. Similar to how people became more sensitive to shaking hands or touching one’s face once those things were made salient as ways to transmit Covid and other diseases.)
Think about water safety regulations again: I don’t really know what they say, and I don’t need to. I just trust that they make sure the water that comes out of my taps is safe. I imagine the story where we achieve a world of clean indoor air would look similar.
Some places where it might be possible to make near-term improvements to regulations and guidelines:
- The WHO Guidelines for Indoor Air Quality mention dangerous chemicals and gases, but not particulate matter or (crucially) pathogens and their transmission potential
- Most buildings in the US fall under ASHRAE Standards 62.1 and 62.2, which do not consider airborne pathogens
- The Occupational Safety and Health Administration in the US can regulate indoor air in workplaces, but its regulations are a little thin on the ground, don’t mention pathogens, and rely on self-certification in most cases
- (sidenote: In other good news, the American Society of Heating, Refrigerating and Air-Conditioning Engineers recently announced that they were committing to developing a national indoor air quality pathogen mitigation standard.), the Biden administration announced initiatives to support clean indoor air, including a revised “Clean Air in Buildings Challenge” listing a bunch of sensible suggested upgrades to air quality, and offering funds from the American Rescue Plan and Bipartisan Infrastructure Law funds. But funds could be more explicitly earmarked for this purpose, as they were planned to be in the Pandemic Preparedness Plan (AP3) which did not pass
Thinking further ahead with a wealthy country like the US or UK in mind, we might imagine:
- Air quality guidelines have been introduced, plus the means to easily monitor air quality. Subsidies are set up for adding filtration, ventilation, and even UVC into homes and workplaces. (sidenote: Niche building regulations: who said effective altruists can’t dream!) are established for new builds
- As a consequence, much like how plumbers will fit houses to a boiler by adapting some of the plumbing, there are also services to adapt houses for cleaner/sanitised air; such as by installing a system of air ducts, rather than just putting a HEPA filter in the corner of a room
Getting started
When we have such a successful precedent in the story of clean water, there is something so transparently worthwhile about this prospect of creating clean indoor air.
I’m not sure I emphasised this enough: if a country installed all the measures I mentioned, it could more or less end respiratory disease in that country. A world in which clean air measures are as widespread as clean water measures are in rich countries is a world which has effectively ended respiratory disease everywhere. It’s just totally possible to stop worrying about a relative catching a cold, or the flu, or pneumonia.
That’s a huge deal: ignoring pandemics, even halving deaths from respiratory disease means saving hundreds of thousands of lives every year. Not ignoring pandemics, the numbers are of course much starker. It’s hard to quantify how bad truly worst-case pandemics could be, given that they could have civilisation-spanning consequences. But these basic measures would help stop or slow many of them.
Like with waterborne diseases, the wealthiest countries will (sidenote: Frontier R&D tends to be concentrated in rich countries, and rich governments are going to be more able to afford expensive public health programs. But also: if utility is sublinear with consumption, then people will be willing to spend relatively more on their safety as they become richer.). A ballpark upper-bound estimate for the cost of comprehensively installing the measures I’ve described in buildings across the US is about $200 billion, or about $50 billion for a more targeted program focusing on buildings (sidenote: Ulrik Horn on the EA Forum points out that pre-schools may be an even more obvious place to focus: “As a parent, kids get sick at an absurd rate in pre-school and it places great stress on the family. Also, it would be super easy to just oneself set up a pre-school with best-in-class air quality in a neighborhood with resourceful parents. These would then spread the word to other parents of how seldom the kids are sick and you can actually create a large business of pre-schools based on having kids that are much less sick.”). But this would surely be worthwhile: even in economic terms, it would save tens of billions in healthcare costs, tens of billions of dollars from lost productivity due to illness, and further further tens of billions from the (sidenote: See the appendix on costs.)
But we needn’t rely on government spending forever and for every part of the plan. Technologies become cheaper when people build lots of instances of them. To give one example, there may come a point where Far-UVC technology is affordable enough to past the cost-benefit test for businesses looking to protect their employees from disease. This is win-win-win territory: employees would prefer to work in an environment where they don’t get semi-regularly sick; employers benefit because fewer employees get sick; and the world benefits because that is one less office-sized petri dish spawning airborne disease for everyone else. In many cases, it’s about supporting a one-time lift to get to that self-sustaining state where everyone’s incentives are aligned.
In short: practical measures to improve indoor air quality seem like an historically good deal.
The story of spreading access to clean water and sanitation is not over. Unsafe water causes more than a million deaths a year — the 13th leading risk factor on one way of slicing things up. Almost all the deaths from unsafe water are concentrated on poor countries, especially sub-Saharan Africa and India. And a solid 25% of the world lacks access to safely managed drinking water. But full access to clean water is no longer encumbered by knowledge about how diseases spread, or how to properly treat water: we have the blueprints. We know how to bring this story to a happy, if belated, ending.
If the project of spreading access to clean water, then let’s do the same for clean air. What’s stopping that from happening? Surely not that it’s impossibly expensive: the cost-benefit analysis already tips in favour for many countries. Nor feasibility: we either already have the technology at scalable prices, or we have clear precedent for similar technologies plummeting in price with R&D. So maybe what’s stopping the story repeating are things like awareness, political will, the visibility of early adopters, and funding for foundational research. And — hopefully — those things are changeable.
More links
- Air Safety to Combat Global Catastrophic Biorisks — Rethink Priorities and 1Day Sooner
- The Plan to Stop Every Respiratory Virus at Once — The Atlantic
- A paradigm shift to combat indoor respiratory infection — Science
- Pandemic prevention as fire-fighting — Works in Progress
- Information on Far-UVC — SecureBio
Appendix: other ways to stop pandemics
I’ve described what it could look like for the world to get its act together on indoor air quality, and begin to deliver clean air at scale, just how most countries in the world deliver clean, safe water almost universally.
A major motivation for caring about this is that such a plan could help end respiratory pandemics. But it’s really worth noting that these aren’t the only tools we have (and which the world at large seems to be underrating) to end that threat. Rather, provisions for clean air would complement other strategies to reach a world which is effectively immune to catastrophic pandemics. Here’s a quick and non-exhaustive list:
- We could develop upgraded ultra-safe PPE, e.g. with air purifying respirators, which is comfortable to keep on for many hours at a time. We can stockpile enough of these systems to enable essential workers across the world to keep basic services running in a worst-case pandemic
- We could build a world-spanning network for detecting novel and pandemic-capable pathogens as they emerge, even when the signs are subtle. (sidenote: Metagenomic (pathogen-agnostic) sequencing.) can be installed to monitor wastewater in populous areas, and as it becomes cheaper it could even begin monitoring the air in busy public buildings with high throughput; ready to pick up on known and unknown pathogens
- We could build the capacity to develop and deploy vaccines, and hand out flexible or universal tests to everyone; curbing human-to-human transmission
I think these measures — especially better PPE and sequencing — could be even more important than the clean air measures I’ve described for stopping worst-case pandemics, because of how specifically effective they could be for that class of threat. But again, these are complementary rather than exclusive options.
Appendix: costs and benefits
Taking indoor air quality seriously would mean spending billions of dollars annually for at least a decade or so. So let’s get quantitative.
First, the costs. Focusing on the US, this report from Rethink Priorities and 1Day Sooner estimates that upgrading the air quality systems in all commercial buildings (at current technology costs) would add up to ~$214 billion total, or ~$10.1 billion focusing just on healthcare facilities and hospitals, or ~$39.2 billion focusing just on offices. On the most (sidenote: The measure being ‘equivalent air changes per hour’, or eACH. Air changes per hour is just a measure of how often air is recycled in a room. UVC doesn’t literally recycle air, but it does make the air cleaner, so the effect can be compared.), upper-room and (sidenote: Assuming the costs of far-UVC fall to become roughly comparable with upper-room UVC.) (sidenote: Considering the amortised cost of installing and running mechanical ventilation; i.e. in terms of both installation and maintenance.), with operational costs less than 20% of ventilation and filtration. I get an estimate of about $78 billion to install Upper-room or far-UVC in every (sidenote: Total US building stock is ~340 billion square feet, of which ~7% are K-12 schools (assuming half of all floorspace used for education) and ~4.7% is for hospitals/healthcare facilities. Assume an installation cost of ~$1500 per ~70m2 room (per this source which gives an estimate for upper-room UVC, and assuming far-UVC falls to be comparable). Multiplying together gives ~$78 billion.). So the headline costs for installing the clean air interventions I’ve described are something like: roughly $50 billion if you’re focusing on the most vulnerable, high-priority public spaces; and roughly $250 billion for a more comprehensive plan. Those estimates are more likely to be conservative than much too high, because they don’t anticipate that costs will fall significantly from today-prices, and they totally could.
Can we try pricing the benefits? The same Rethink Report makes a rough estimate that plans on the more comprehensive end of what I’ve described could reduce overall rates of transmission of respiratory disease by just under 70%.
First, there’s the cost from non-pandemic transmissible diseases. This breaks down to the morbidity cost of not being able to work (lost wages), the direct cost of healthcare, and in worst cases the mortality cost. This 2000 report estimates that infectious diseases account for 15% of US healthcare spending, which in 2020 accounted for about 14% of US GDP (combining public and private spending). US GDP is about $23tn. Let’s conservatively guess that 10% of that burden could be eliminated by properly treating and sanitising indoor air and surfaces. That would suggest a saving from the direct healthcare costs of $23tn × 15% × 14% × 10% = roughly $50 billion. Figuring out lost wages is tricker (I couldn’t find a direct estimate in 10 minutes of looking). The ONS suggests that the sickness absence rate in the UK is about 2%, which we can assume is roughly the same in the US. Let’s again assume that 20% of these sick days could be prevented by significantly upping our game on killing germs in indoor spaces. And we’ll assume that the elasticity of total working days to GDP is about 0.2 (increasing working days by 1% increases GDP by 0.2%). That gives a BOTEC of the losses from diseases preventable by fixing indoor air and surfaces of: $23 trillion × 2% × 20% × 0.2, which roughly equals $20 billion.
Then there’s pandemics. The Institute for Progress estimate the overall cost from Covid to the US at around $10 trillion. Conservatively assuming a yearly likelihood of a pandemic at least as bad as Covid of 2%, that suggests the US faces a yearly expected cost from the risk of pandemic per year of at least $200 billion. The amortised annual cost of the program we’ve described would be about $20 billion per year for a decade or so, meeting the cost-effectiveness bar if it reduces that risk by (sidenote: Another angle: the expected cost to the US from one percentage point of risk of a pandemic at least twice as bad occurring within a given time period (say 50 years) is at least $200 billion. It seems entirely plausible that the program described would reduce that cumulative risk by at least a percentage point for around $200 billion.).
That’s not mentioning the costs from impaired cognition caused from poor air quality, which (sidenote: I’m still a bit confused by the literature on cognitive costs of poor air quality, but it seems like the effects of stuffy indoor air on day-to-day productivity are real and possibly quite large. This study assessed the effect of C02 concentration on performance on tasks designed to measure “complex cognitive functioning in ways […] relevant to the tasks of workers in buildings”. Eyeballing the results, it looks like the drop in performance from relatively clear air (600ppm) to a fairly stuffy office (1000ppm) led to a 11–23% drops in the raw scores on these tests (about 15% on average), and the drop from fresh air to ~a very stuffy meeting room (2500ppm) ranged from 44 to 94% across the tasks. N=22 and I’m coming at this with a skeptical prior, so I’d guess the real effects of C02 are smaller. But if they’re in the same ballpark, then there are some huge gains to be made for just making sure indoor air is fresher. You can see more discussion on this LessWrong post, including this mini literature review from Gwern. This study and this review also find significant effects.); or the cost to health from non-pathogenic matter like small particulates.
If the spending numbers sound like a lot, consider how much the US is prepared to spend on fire safety: around $273 billion in 2014. And the majority of that spending is directly comparable to the air quality improvements I’m discussing: things like installing sprinklers, installing alarms, and using fire-resistant materials in buildings and products. Covid alone caused five times more deaths than all fires in the last 45 years combined. The implication is not that we’re overspending on fire safety (not sure if anyone holds that take strongly) but that if it is worth it to spend hundreds of billions on fire safety measures every year, then it’s probably worth doing the same for indoor air quality measures. Or consider that the US is prepared to spend well over $500 billion annually on defence spending (relevant because defence against pathogens is also a kind of national defence). Or more than $200 billion annually on counterterrorism over the past decade or so.
Speaking more speculatively: I see a significant difference between spending on clean air on one hand, and examples like fire safety, counterterrorism, and national defence (military) spending on the other: (sidenote: Commenter ezrah on the EA Forum points out that this is a notable disanalogy between clean air and clean water. In their words: “Clean water systems need large investment in infrastructure and government implementation upfront, as much as they need more technological advancement, since Clean Water is a public good. Indoor Clean Air, or at least the solutions you described above, don’t need large infrastructure or government investment. The quality of the air in my house or office is a private good. The private market can develop the R&D and market directly to consumers, without the need for the government to step in, as long as there’s consumer interest. The fact that the TOC [theory of change] for Clean Air Indoors doesn’t need to go through government makes me more optimistic about success (although of course if there are government standards and gov R&D spending, it will go faster). On the other hand, perhaps Indoor Clean Air is more similar to lead paint regulation, where the individual consumer isn’t aware enough of the dangers and benefits, even though theoretically it’s more lucrative to sell safe paint than poisonous paint.”). If the cost to install e.g. far-UVC in a workplace falls, then it’s easy to imagine an increasing number of workplaces becoming willing to pay the full sticker price, just to recoup the opportunity cost of sick leave (and because employees might begin to demand that their working environment isn’t one where they’re exposed to a constant risk of getting sick). For potential buyers willing to pay less than the sticker price to install clean air measures, a government would only have to subsidise the difference to buy all the externalities (like all the people going home from work not spreading disease on the subway). By contrast, a business is unlikely to choose to donate to their local fire station out of sheer self-interest, because they’d capture too small a fraction of the benefits.
Coloured etching by W. Heath. Desription: “A woman dropping her tea-cup in horror upon discovering the monstrous contents of a magnified drop of Thames water; revealing the impurity of London drinking water.” ↩︎
The silent highwayman : Death rows on the Thames, claiming the lives of victims who have not paid to have the river cleaned up, during the Great Stink. ↩︎
Cholera “Tramples the victors & the vanquished both.”. Description: "Cholera, as a large shrouded specter with skeletal hands and feet, indiscriminately crushes soldiers on both sides of the battlefield. " ↩︎
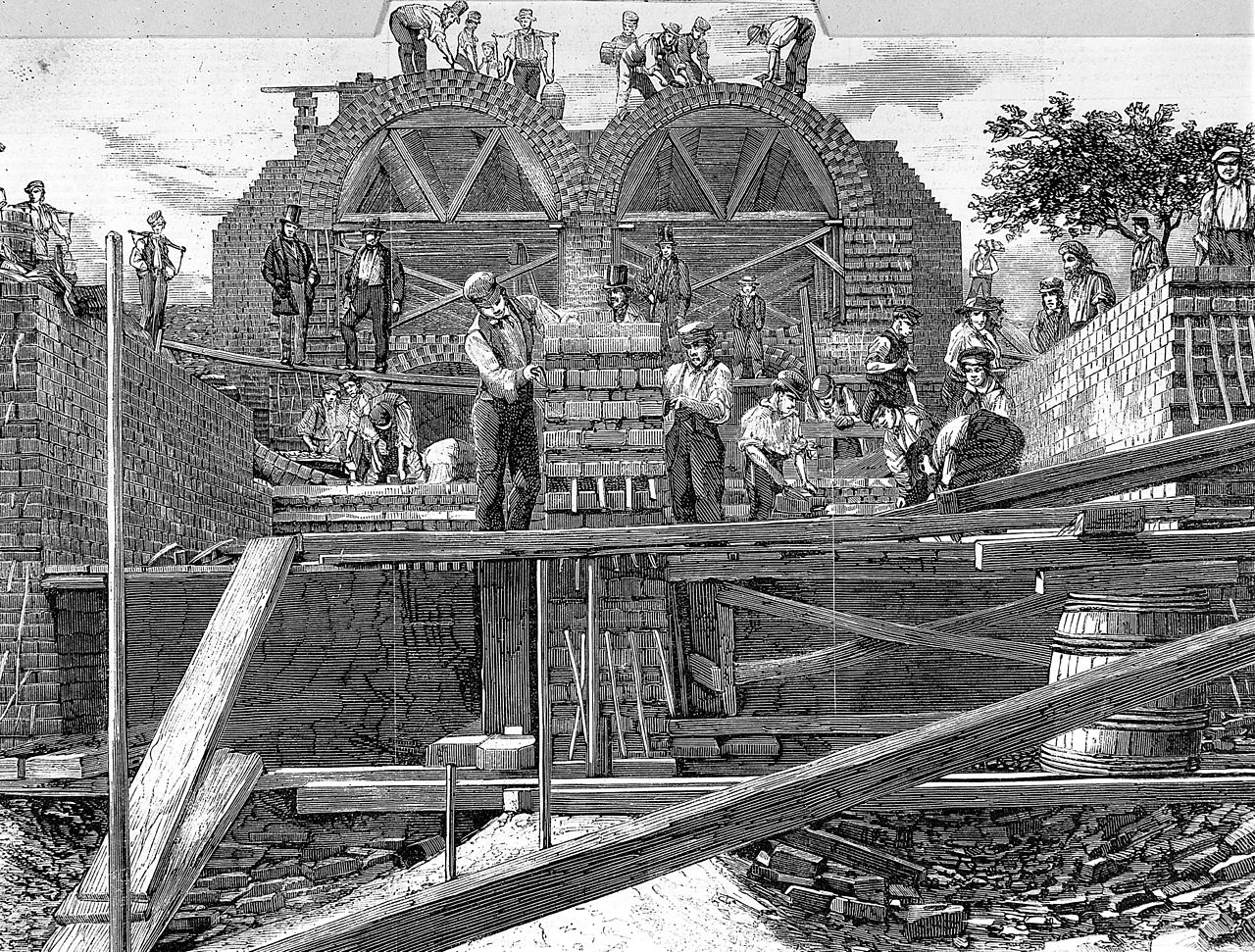
The main drainage of the Metropolis. Description: “sectional view of sewerage tunnels from Wick Lane, near Old Ford, Bow, looking westward” ↩︎
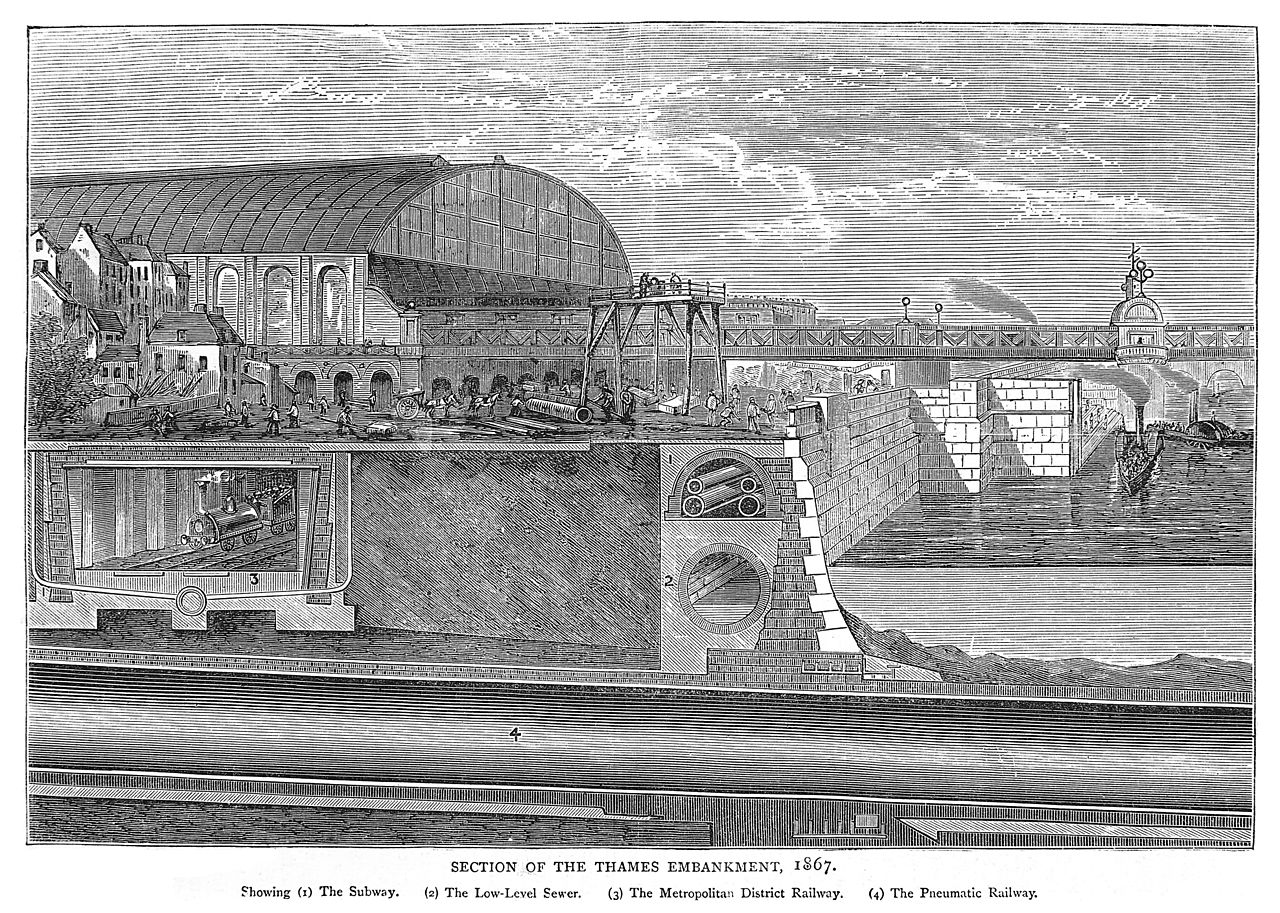
Installation of the sewerage system of the Metropolis. Description: “Installation of the sewerage system of the Metropolis, The Thames Embankment in section beneath Charing Cross Station (1867) showing: (1) underground conduit carrying water, telegraph cables and gas mains; (2) low-level intercepting sewer; (3) Metropolitan District Railway subway; (4) Pneumatic Railway. The wall was built as much as 500 feet into the Thames, creating 37 acres of reclaimed land.” ↩︎
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Back to writing